

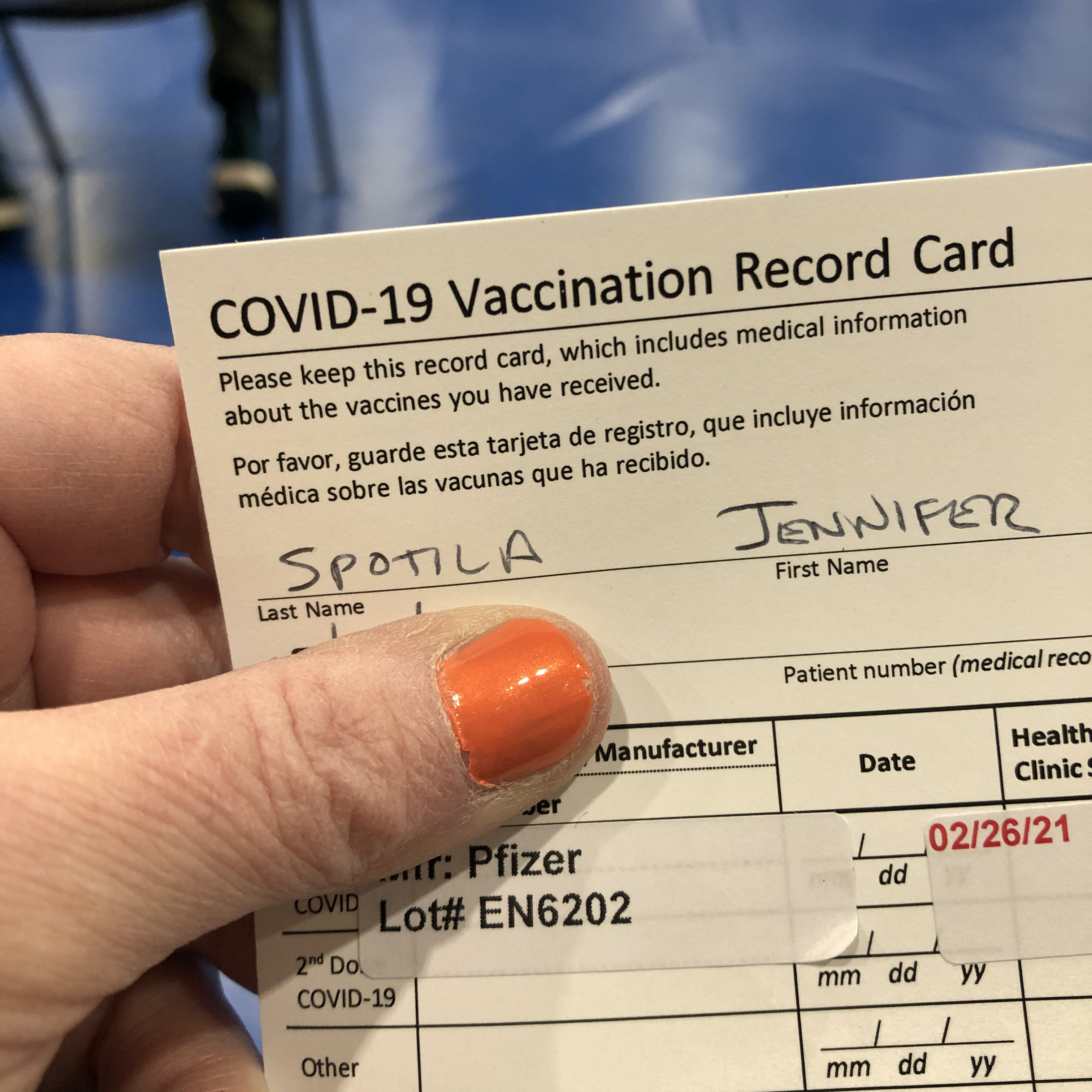
On Friday, I got my second dose of the Pfizer COVID-19 vaccine. The vaccine side effects were definitely more intense this time, but not unmanageable. I am so glad I was able to be vaccinated, and I am documenting the experience so that other people with ME can get a sense of what to expect.
My husband and I had no difficulty scheduling our second shot. The date was set by the county, four weeks after the first dose, and delivered at the same clinic location. Once again, my husband and I were able to get appointments in the same time slot.
As I had before the first shot, I took an extra dose of my H1 histamine blocker one hour before. I have mast cell activation syndrome, and The Mast Cell Disease Society recommends that patients premedicate with their H1 blocker in this manner. I also skipped my beta blocker the night before, on the advice of my doctor. Be sure to check with your doctor about any changes to your medications prior to vaccination.
Upon arrival at the high school vaccination clinic, I noticed two things right away. First, there was an increased police presence compared to our first time. I don’t know if that was due to the mass shootings in Atlanta and Boulder, or due to the number of people they expected onsite that day. Second, there were a number of wheelchairs parked at the entrance, and I later saw a volunteer pushing someone through the line in one of them. I was really happy to see that these were available for people who might not usually need a wheelchair but who would be unable to walk around the clinic site.
Another improvement was the clear marking of walking lanes and distance markings. Volunteers gave better instructions about where to go. The logistics seemed to be smoother. Our actual waiting time for registration and then vaccine administration was shorter than last time as well. The observation area had also been improved. The high school bleachers were folded up and the entire area was dotted with plastic chairs in ones and twos.
Getting the shot was quick and completely painless. The volunteers have optimized the whole thing for maximum efficiency. Syringes are pre-loaded. One volunteer handled data entry and marked my vaccine card, while the nurse asked a few questions about whether I had ever reacted to a vaccine. Even the bandaids to cover the injection site were partially opened and waiting in a line on the desk. The whole thing went so fast that I hardly had time to thank the nurse and volunteer.
While we waited in observation, my husband turned to me and said, “Where’s the nearest Krispy Kreme?” (We had to look it up, and the answer was 30 minutes away. We didn’t go.) After I texted a picture of my vaccine card to my family and friends, I spent a few minutes just watching everyone in the high school gym. The noise echoed around the space, and most people seemed to be in a good mood. I thought about the video of Yo-Yo Ma playing at his vaccination clinic after receiving his second dose. As the nurse who administered his vaccine said, “It just brought that whole room together. It was so healing.” We need that in every clinic! What a tremendous gift immunized musicians could give to their communities. I think it could do more than lift the mood of everyone present. Vaccination is not just a personal healthcare decision. It is an act of love for each other. Perhaps music could help us feel that in a way that the necessarily fast-paced mass vaccination clinic environment does not.
After our self-timed 15 minutes was up, we thanked the volunteer in the observation section and headed to our car. It wasn’t until I got to the parking lot that I started to cry. It finally hit me: my husband and I are going to be ok. Ever since March 2020, when I read this first-person account of caring for a spouse with COVID-19, I have lived in terror of my husband getting sick. The COVID-19 vaccines available in the US are highly effective at preventing people from getting COVID-19. And no one who received a vaccine in the clinical trials was hospitalized or died of COVID-19. It is true that there is a lot more to learn about the long-term effectiveness of the vaccines, but for now I am confident that neither of us will get seriously ill from COVID-19. The relief of that hit me, and I cried.
When we got home, I had to pay up on a bet. Late last year, my husband and I made a bet about when we would be fully vaccinated. I said it wouldn’t be until summer. He said we would be vaccinated by April 1st. The prize was a batch of homemade chocolate chip cookies. My husband doesn’t bake, and I was really looking forward to watching him learn to make cookies. But I lost! I knew, based on my experience with the first vaccine dose, that the side effects would hit me quickly. I planned ahead and made the cookie dough the day before, and as soon as we got home, I scooped it out and baked the cookies. (Homemade chocolate chip cookies are better than donuts anyway, don’t @ me.) That was a smart choice, because the side effects did not wait long.
Less than four hours after receiving the vaccine, I felt a crash coming down on me like a heavy curtain weighing thousands of pounds. I had trouble putting coherent sentences together, and I couldn’t read or knit. My resting heart rate was elevated at least 15 beats per minute higher than normal. I listened to some music, ate some dinner, and went straight to bed.
The first vaccine dose had given me muscle and joint pain, as well as severe malaise for about 36 hours. The second shot caused pain in my lymph nodes under the dose arm, as well as overall muscle pain. I was feverish, and awoke with night sweats the first night. The muscle pain was severe enough to wake me up the next morning, and prevent me from napping all day. My resting heart rate was still higher than normal, but not as elevated as the hours right after the vaccine. I also had difficulty staying upright, even in a recliner, although that did improve as the day went on. In the evening, I had an episode of vasovagal syncope without fainting, possibly triggered by gut cramping.
When I’m crashed, I feel like I’m wearing a football helmet and pads made of concrete. That feeling persisted into the second day, even as the other vaccine side effects improved. I couldn’t do any of my routine tasks, and the heavy aches stayed with me. It was a difficult weekend. Fortunately, my husband had no side effects at all.
Every day since has been a little bit better. My arm still hurts sometimes, and my headache comes and goes. It’s now five days since my vaccination and I think I am about back to baseline. That’s worse than a healthy person would expect, but not the worst case scenario I feared.
I strongly encourage people with ME (and the people they live with) to consider getting vaccinated for COVID-19. Based on my experience, and that of my friends with ME, the side effects are intense but not unbearable. Crashing for a week is far better than moderate to severe COVID-19. That being said, please consult with your doctor before making the decision. You may need to adjust medications prior to vaccination, especially if you have mast cell activation syndrome. Your doctor is best placed to advise you on your individual circumstances and whether you are well enough to take the vaccine. I know at least one ME patient who has been advised to wait, so discuss your options with your doctor if you have any concerns at all.
These vaccines are an incredible achievement. Prior to COVID-19, the fastest vaccine to market took four years. It’s frightening to imagine the death toll if we had to wait three more years for a COVID-19 vaccine. To have vaccines this effective, this safe, and this quickly is proof of what we can achieve when we invest the money and the effort in a scientific problem.
There is one more thing I need to do to ensure I am fully immunized against COVID-19: I have to wait. A person is not considered fully immunized until two weeks after the second dose of Pfizer or Moderna’s vaccine. And once I hit the two week mark? I am going to hug my Dad for the first time since February 2020.
Thank you, Science. Thank you.



The Death Threat Myth Exposed
Update April 7, 2021: Further comment from Dr. Vicky Whittemore added to the end of this post.
Last week, an old story was recounted to a new audience. During the March 30, 2021 NIH telebriefing with the ME/CFS community, Dr. Vicky Whittemore said that there had been death threats against grant reviewers in the past, and that this was one reason why NIH is now withholding the names of reviewers on the ME/CFS Special Emphasis Panel (referred to as the “SEP”). This is not the first time that NIH has used the story of death threats to justify withholding the grant review rosters from the public. This excuse is overblown, and every repetition of it harms the ME/CFS community by perpetuating derogatory stereotypes of advocates and people with the disease.
I can say that the death threat story is exaggerated because I have documentation of what actually happened. I began investigating who serves on the ME/CFS SEP in 2012. Grant review panels are federal advisory committees, and the law requires that the membership of the committees be disclosed to the public. Despite this requirement, Don Luckett at the Center for Scientific Review told me in 2012 that they no longer posted the rosters online “due to threats some previous panel reviewers have received.” At his suggestion, I filed a FOIA request for the rosters, and I also requested evidence of the threats. NIH initially refused to release the information, but I appealed and in 2014 I won. NIH released the rosters to me, along with the evidence of the threats cited by Mr. Luckett.
Despite Luckett’s use of the plurals “threats” and “reviewers,” the documents show that there was only one isolated incident. Dr. Myra McClure, a retrovirologist from Imperial College London, was scheduled to serve on the SEP on February 22, 2011. On February 5th, she wrote to the Panel’s Scientific Review Officer:
Dr. McClure did not express fear or alarm in her email. Instead, she referred to the call as “bullying/intimidation,” and withdrew from the Committee because, “I am too busy to put up with nonesense [sic] like this.”
Two days later, Mr. Luckett forwarded McClure’s email to a colleague with the following summary:
The SEP meeting was subsequently canceled. A new panel was recruited and the meeting was held without incident on March 24, 2011.
To be clear, NIH decided to withhold the names of grant reviewers from the public despite the legal requirement that the names be disclosed. Federal advisory committees do their work in public, and committee members know that their names and contact information will be disclosed to the public. Nevertheless, NIH withheld the names for years, thereby shrouding the operation of the SEP in secrecy and preventing the public from assessing who was reviewing ME/CFS grants.
I can imagine a situation where death threats could be so specific, targeted and frequent that it may warrant special precautions of some kind. But that is not the case here at all. The sum total of evidence of “threats against reviewers” amounts to a single phone call in 2011 to a single reviewer, relaying a story of “extremists” with guns who were supposedly going to march on NIH and CDC at an unspecified date and time. As unpleasant and annoying as the call was to Dr. McClure, the statements do not appear to meet the criminal definition of a death threat. Her description of it as bullying and intimidation is much more accurate. And that’s all there is. There were no other threats; there are no extremists. It goes without saying that no one obtained guns and marched on NIH or CDC. Yet ten years later, NIH is still citing this incident as justification for withholding information from the public.
It’s easy to trace how the story of that single phone call to Dr. McClure was repeated and magnified over time. After I made my initial inquiry about the SEP rosters in July 2012, there was email correspondence among several people at NIH’s Center for Scientific Review. Included in a batch of material “relevant to why we’d prefer the ME/CFS rosters not be made public” was an August 2011 article from The Guardian relating stories from researchers in the UK about hate mail, crank calls, and at least one disturbing personal interaction. The article uses words like “extremists,” “militants,” and “dangerous,” but includes no evidence of any coordinated group or campaign. McClure’s withdrawal from the SEP is referenced in that article, but now it is described as “she had to withdraw from a US collaboration because she was warned she might be shot.” That is quite a bit more specific and disturbing than the way she described the phone call immediately after it happened.
Fast forward ten years to the ME/CFS telebriefing last week: Dr. Whittemore referred to the death threat story while delivering her update on grant review. She was discussing why NIH is not publishing the ME/CFS Special Emphasis Panel rosters, and she said:
Dr. Whittemore, like Mr. Luckett in 2012, said “threats” and “reviewers,” when the documents show there was only one isolated incident. And once again, NIH is saying those “threats” justify withholding SEP meeting rosters.
I reached out to Dr. Whittemore for comment, and asked for details about the threats she mentioned. She replied,
Dr. Whittemore made her comments last week based on a story she heard from someone else at NIH, a story which she says contained no specifics. This makes me wonder how often this story gets repeated at NIH, and how much it informs the way NIH sees people with ME. The story is still being told, and is being used as an excuse to withhold information from the public. That certainly suggests that NIH believes some ME/CFS advocates could be dangerous–otherwise, why would a story from ten years ago be so significant.
I spoke with several advocates, all of whom said that Dr. Whittemore’s repetition of the death threat story is harmful. Sharon Shaw told me the comment, “portrayed the ME/CFS community as dangerous and unstable. . . Comments like this vilify the ME/CFS community, and further stigmatize and disparage people living with ME/CFS.”
Advocate Kellyann Wargo told me:
That idea was echoed by Denise Lopez-Majano, who said, “How can we trust NIH has our best interests at heart if they say things like this? If NIH is perpetuating this belief among themselves, how can they expect to encourage new researchers to enter the field?”
I asked Dr. Whittemore how she would respond to the concern that her comments could perpetuate the myth that people with ME/CFS are unstable and/or dangerous. She replied, “I am sorry that my comments may be harmful to individual [sic] with ME/CFS. This was not my intent.”
The death threat story has taken on a life of its own. One crank call to one reviewer in February 2011 became “threats to reviewers” that NIH still believes is sufficient justification to withhold the rosters of ME/CFS SEP meetings. NIH continued to use that justification for two years after I won my FOIA appeal. The story was repeated within NIH over the course of ten years, including to Dr. Whittemore. She then went on to repeat the story to the ME/CFS community as part of the reason why NIH once again decided to withhold the membership rosters of the ME/CFS review panels.
The repetition of this story by a leading member of the Trans-NIH ME/CFS Working Group does real harm. Dr. Whittemore’s comments lent gravitas to the stereotype that people with ME are mentally ill and dangerous, and makes it sound like there is still a threat to be concerned about. Dr. Whittemore presented the story as established fact–despite the fact that this single phone call occurred ten years ago; despite the fact that there is no evidence of “extremists,” “militants,” or any violent intentions among ME advocates; and despite the fact that she herself has no specifics about what occurred and when.
In light of the full picture, it appears to me that there is a persistent prejudicial view of ME advocates at NIH. Furthermore, it is obvious that NIH should not continue to recycle this story for any reason, including as a justification for preventing the ME community from evaluating who reviews ME/CFS grant applications.
Update April 7, 2021: Dr. Vicky Whittemore provided additional comment: