
My friend, Jenny R, wrote these profound words about her sickaversary.
 10 years and 4 days ago today I got sick and never got better. I wrote this to commemorate it:
10 years and 4 days ago today I got sick and never got better. I wrote this to commemorate it:
I want to write something incredibly profound and moving for my 10 year sickaversary. But I can’t. Writing used to be my outlet. It was something that came easily for me and I was proud of my talent with words. Business school beat my affinity for flowery and often turgid prose out of me in favor of conciseness and bullet points. But even so I still retained a nugget of my craft and found ways to enjoy penning a tax research paper in place of angsty poetry.
I could say that it happened the second the virus entered my bloodstream. That a microbe found and destroyed my skill in a summary execution. And in some ways that is true. But it was a slower and (at times) more devastating death. The virus/CFS hijacked my focus and memory immediately. A year later migraines and their medications took and continue to take my words (a condition called aphasia). Then for good measure they took my ability to type or write without angering the ruthless dragon that is the permamigraine (occipital/trigeminal neuralgia). More recently nerve compression from herniated cervical discs and stenosis keep my hands from working properly. But even without these numerous, concrete medical issues, the fact is that I lost faith in my mind a long time ago. That kind of self doubt is as debilitating as my motor deficits.
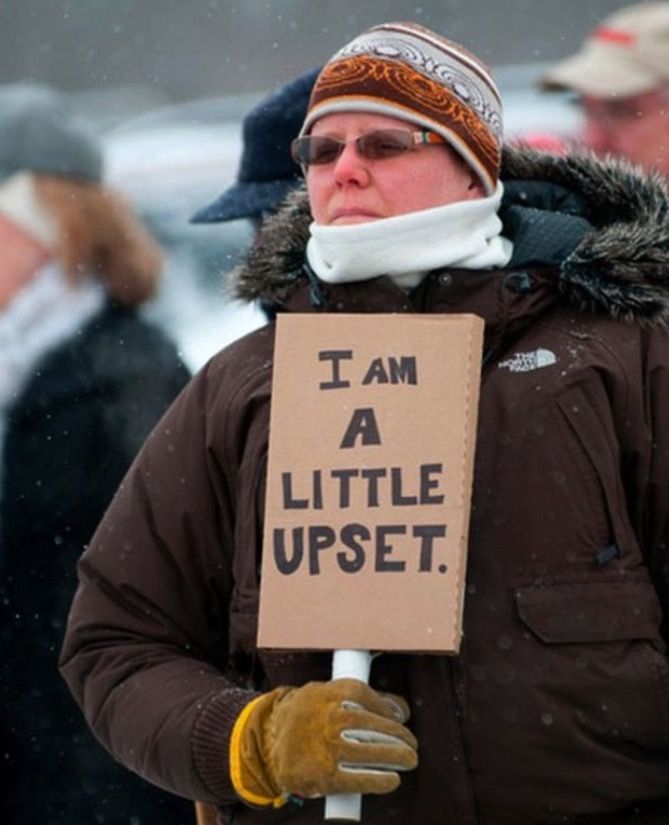
Because no matter what happened in my life – whether I was single or attached, fat or thin, rich or poor, happy or sad – I had my intellect. Twenty years ago when I graduated from high school I was awarded Most Likely to Run for President and bound for one of the best business schools in the country. I knew I was smart and I felt like because of it endless possibilities awaited me. I was told all my life if I studied hard that everything would work out. Above is a picture of me at 18. Her innocence and joy are hard to look at because I know she would be heartbroken if she knew how it all worked out. That the girl who wanted to major in literature struggles to focus on a young adult audiobook now. That the former CPA who used to run audits can hardly balance her checking account anymore.
This is usually the time where I start to worry I’m alienating people with the harsh truth of living life with a debilitating illness. The part where I list the joys that are still plentiful in my life. The part where I feel pressure to say that I’m grateful for getting sick because it made me see beauty where I once did not. That now I know what really matters in life. So it’s all good.
But I won’t do that this year. It’s been 10 fucking years. I have every right to be angry that I’ve spent 10 years in bed. That I watch my friends and family travel, get married, have kids, excel in their careers, and move forward in life. I feel stuck. Trapped in amber. Preserved at the age of 27 except with more lines on my face, gray hairs, and a crappier metabolism.
Of course I know it could be worse. I am friends with people much sicker than I am. I have friends who have died. I’m a white girl in America with parents who can afford to help her. My privilege abounds. But because of the plentiful cheery disabled person tropes, people’s discomfort with their own mortality and the pain of others, our positive attitude focused culture, and the ingrained socialization women receive to be pleasant and meek, I have subjugated my own grief time and again over these last 10 years. So for today I’m sharing it with you. I’ll resume regularly scheduled Stepford programming tomorrow.
But I’d be remiss to say that my life of perpetual pain, fatigue, and loss is devoid of love and joy. It’s so not. I’ve got a kick ass boyfriend who genuinely enjoys taking care of me instead of doing it out of obligation, friends who never give up on me even when I disappear down a migraine hole for months, a niece and nephew that don’t see a sick person just their purple-haired Aunt Jenny, parents who let me and my cats move in and disrupt their swinging Empty Nest life without hesitation, a little sister who in many ways has become my big sister by taking care of me whether than means pedicures or help with errands, a Bestie/Braintwin who knows Jensen Ackles and the cuddles from Corgis can cure anything, my late babycat Cameron who was always up for spooning and never stopped trying to groom me, and a wee tortie Callie who is perfectly happy to spend her days in bed with me. These people love this Jenny. Even if she is broken.
I want to sum this up with some amazing wisdom I have gleaned from these last 10 years but all I can say is that it really sucks to watch everything you thought made you…well…you disappear into a fog of fatigue and relentless pain. It is devastating to watch what you hoped for the future, in my case a life of professional success, exciting travel with a loving husband, and maybe even a kiddo or two, disappear down the drain. The grief never really ends – it just ebbs and flows.
But it doesn’t mean I don’t have hope, gratitude, joy, love, and even excitement in my life. Doctors have found consistent, biological differences in CFS patients and the questionable studies that relegated it as a somatic disorder that only psychotherapy and exercise could cure are being disproven. I’m going to see the Old 97s play next month and am hoping for a trip to Colorado at the end of the summer to explore canniboid oil for pain relief.
So my great wisdom is that I don’t have to pigeonhole myself as the smiling disabled person who puts everyone at ease and is full of folksy wisdom. But I also don’t have to live solely in my pain, day in and day out. I can be grateful and grieving at the same time. I can look forward to tomorrow while being sad for that hopeful 18 year old girl that didn’t expect this future. To quote the 11th Doctor, “The way I see it, every life is a pile of good things and bad things. The good things don’t always soften the bad things, but vice versa, the bad things don’t always spoil the good things and make them unimportant.” Or better yet, to quote the TARDIS, “[Human beings are] so much bigger on the inside.”









Book Review: Through the Shadowlands
I have read this book from two perspectives. First, I had the opportunity to read Julie’s early drafts and provide feedback as her friend. But before publication, I was able to read the final version from start to finish with the perspective of a reviewer, and I offer my comments here.
The first thing to know about this book is that Julie can write. She tells her story with honesty and clarity, and the narrative tugs the reader along her winding path from childhood through illness and on to the other side. Julie can explain facts and details so clearly, and then write passages like, “The straw of my house gleamed golden against the brown patches of mud plaster, as if the house were the love child of the sun and the earth.” The experience of reading this book is a pleasure.
Julie’s story of getting sick, and how her life began to shrink, will feel very familiar to people with ME. She describes knowing, “Something is really, really wrong with me.” We’ve all had that moment – before diagnosis, perhaps even before seeking medical care. Each of us has that point of recognition that our bodies have shifted out of health in a serious and fundamental way. And Julie entered the same labyrinth that so many of us did: the trips to different doctors, the suggestion or diagnosis of a psychological problem, the lack of scientifically established treatments. She faced victim blaming, where someone insists that if the suggested treatment didn’t work then she must not be trying hard enough, or must not want to get well. We’ve all been there.
But Julie isn’t just talking to ME patients with this book. In fact, I think she is talking primarily to people not familiar with ME. That audience will feel, along with Julie, what this is like. She writes, “I tried to explain that running off after every quack treatment my friends pushed on me just made me feel desperate and hopeless. The reality was that nobody knew what to do about this fucking disease — if they did, I would have heard about it by then.” I wish I could have been so clear with the dozens upon dozens of people who have tried to push answers on me over the years.
Despite choosing to accept her reality, Julie does not stop looking for answers and rejecting ideas that do not make sense to her. Supplements are a way to part the “gullible” from their money. She found people who wore magnets in their underwear or relied on homeopathy or wore devices that zapped electricity through the wrist. But other ideas do not sound so strange to her, like a shamanic journey or mold avoidance or consulting a psychic.
And this will be one of the challenging parts of Julie’s story for people to accept. Realizing that science was not going to provide her with answers, she decided to try a “Hail Mary pass” and test whether mold was making her sick. She chose mold based on her intuition. For some reason she cannot articulate, trying mold avoidance felt right when magnets and supplements sounded wrong.
After spending two weeks in the desert, Julie finds that she does react immediately and strongly to mold (or something else in the environment). And showers bring near instant relief from the worst of the symptoms. Over and over, she experiences sudden, crippling attacks and is restored by showers or other decontamination methods. Julie deftly explains the science behind mold reactivity (while noting that so much more science is needed), and theories for why her reaction could be so severe and resolve so dramatically. There is no proof beyond her self-experimentation, but there can be no denying that this is true for her.
Julie’s mold avoidance actually increases her sensitivity, and the severity of her reactions. There are a number of frightening episodes, but she clings to the fullness of life as she navigates through them. Despite her illness, Julie resumes her career, meets a new man, and travels internationally. I think she shows extraordinary courage, living her life and trusting that she will be able to handle whatever the illness throws at her.
One of the remarkable things about Julie’s story is the way she balances seemingly inconsistent points of view. She tackles mold avoidance scientifically, but also holds herself open to emotional and spiritual approaches. She is constantly questioning herself and her interpretations of her experiences. Julie is willing to try things, even if they sound a little wacky, and then thoughtfully integrate what she learns. This is an extraordinarily difficult thing to do, and even more difficult to explain well. Julie does both. Through experimentation, Julie is able to reduce her reactivity to mold and regain much functionality. She is not cured, but she is much improved.
Mold avoidance is controversial, both inside and outside the ME community. And Julie is clear that, “My experience obviously does not establish that ME/CFS as a whole is caused by mold or related contaminants, and I strongly doubt that’s true. Accurately assessing how many ME/CFS patients are affected by mold is impossible at this point.” Julie is simultaneously adamant that there is a scientific basis to mold sensitivity, and that much more science and funding is needed to find answers for all ME patients.
Through the Shadowlands speaks an important truth to the world. Julie tells the truth about what it is like to live with ME in ways that patients will identify with and that outsiders will understand. She makes the case for why current medical care and PACE-like models are atrociously bad. And Julie’s determination to seize life to her fullest ability is an example of courage to everyone.
My favorite parts of Through the Shadowlands are the passages where Julie describes her connection to the earth. I have always felt a deep well of connection to nature, and I recognize the same in Julie’s description of her time in Death Valley:
Through the Shadowlands is an honest and moving account of what it is like to have ME, and to live a real life with it. In my opinion, both the ME community and those who have never heard of us can learn something from Julie’s story.