
NIH funding for ME/CFS research should be increasing each year. Everyone agrees that this is needed. Instead, 2020 funding has flatlined. Worse yet, we are in danger of falling off several cliffs looming ahead.
Image credit: Off the Charts, AJN
The 2020 Numbers
Based on currently available numbers, NIH spent $11,696,985 on investigator-initiated grants and the Collaborative Research Centers in FY2020 (see note 1) That is basically flat with 2019 and 2018 spending. Here is how 2020 compared to 2019. (I have previously covered the details of 2019 spending and a subsequent fact check).
| FY 2019 | FY 2020 | % Change | |
|---|---|---|---|
| Extramural $ | $4,627,302 | $4,612,339 | -0.3% |
| Research Centers | $7,381,515 | $7,084,646 | -4% |
| Total | $12,008,817 | $11,696,985 | -2.6% |
There were eleven extramural projects in 2020. Seven continued from 2019: Abdullah, Davis, Li, Nacul, Rayhan, Unutmaz, and Younger. Williams received a five-year renewal of his grant. On behalf of IACFS/ME, Friedberg received a small grant for the organization’s meeting, originally scheduled for June 2020 and to be applied to a future meeting (see note 2). Two new five-year grants were awarded t0 Jason and Shungu. The Research Centers are the same from last year: Columbia, Cornell, and Jackson Labs. Data Management Center: RTI.
Once again, NIAID and NINDS provided the vast majority of funding (83%) across all categories. Eight additional Institutes contributed the remaining 17%, although two of those only contributed a few thousand dollars to the IACFS/ME meeting. NIAID split its funding almost evenly between grants and Centers, with 53% going to investigator-initiated grants. NINDS spent 59% of its funding on the Research Centers, and the remainder on investigator-initiated grants.
Three grants from FY2019 came to an end without additional funding in FY2020, as expected: Daugherty, Friedberg, and Light. Last year, I expressed concern that if the five-year grants to Friedberg, Light and Williams (who was scheduled to end) were not renewed or replaced, investigator-initiated funding could drop by 34% in FY2020. Fortunately, Williams renewed his funding. The new R01 grants to Jason and Shungu helped keep the total funding number steady.
Which institutions and investigators are getting the most money? These six investigators received 78% of the total FY2020 funding:
- Jackson Labs/Dr. Unutmaz: $2,771,471
- Cornell/Dr. Hanson: $1,916,014
- Columbia/Dr. Lipkin: $1,900,660
- RTI: $1,149,560
- Stanford/Dr. Davis: $750,389
- DePaul/Dr. Jason: $613,912
Extramural Cliff
At first glance, maintaining our level of funding from 2019 to 2020 sounds like good news, especially given the once-in-a-century challenges of 2020. It sounds even better to say that $11.6 million is 74% higher than 2015, and the Research Centers did not even exist then. Note: I am not including intramural funding in this calculation.
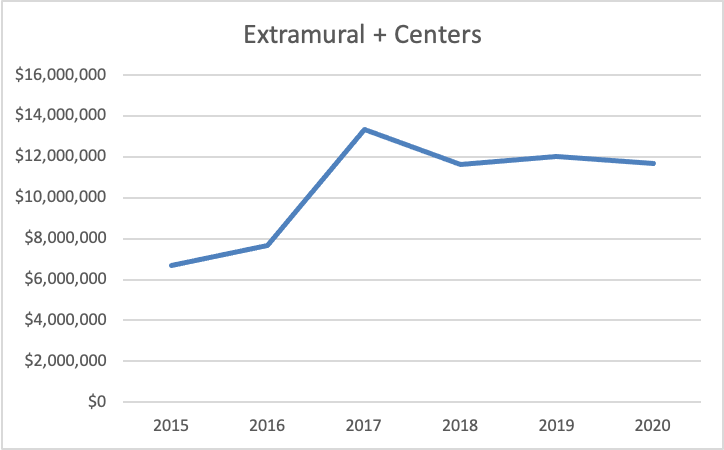
The overall trend looks pretty good. Unfortunately, it is not that simple. The problem is the drop in funding since 2017 and the reasons for that change.
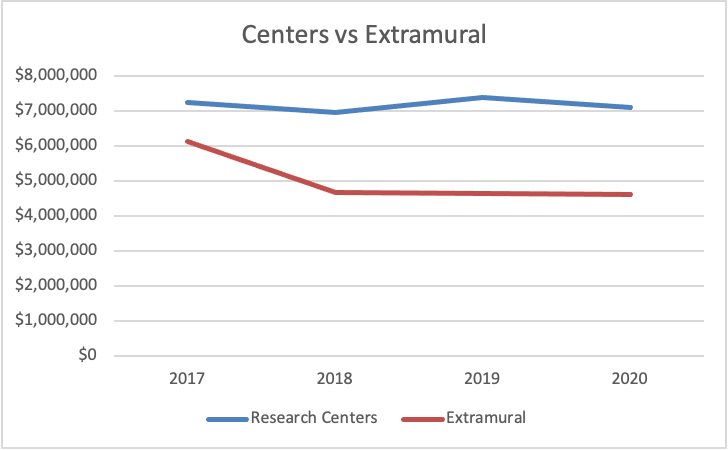
In FY 2017, ME/CFS research funding for extramural grants and the Research Centers reached its peak of $13.3 million. In FY 2020, funding was down 12.5% to $11.6 million. What accounts for that decrease? It’s not the Research Centers, because that funding hasn’t fluctuated more than about 5% up or down. The reason ME/CFS research funding is down from 2017 is because of the precipitous drop in extramural grant funding.
I pointed this out last year when I said ME research needed life support. It’s still true. Funding for standalone investigator-initiated extramural projects has been dropping for years. Let’s take a closer look at the extramural funding trend since 2015.
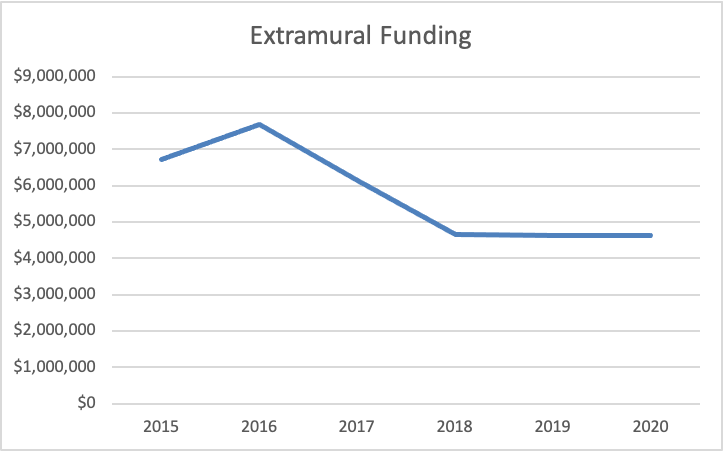
The peak of extramural funding was in 2016 at $7.7 million, an increase of almost 15% over the previous year. The reason why funding was so high in 2016 was the administrative supplement funding provided to seven investigators. The availability of this funding was announced in April 2016, a full five months after NIH promised to “ramp up” its funding of ME/CFS research. The supplements were a quick infusion of research dollars, but it was always intended to be a one shot deal.
It was a good thing NIH did this, because it was another 17 months before the Research Center awards were announced. If NIH had not provided the $1.2 million in administrative supplements, 2016 extramural funding would actually have been 5% lower than 2015. That would have put NIH in the awkward position of announcing it would increase funding and then have funding drop.
In any event, the supplements expired after one year and so extramural funding dropped by 20% in 2017 to $6.1 million. If the only factor driving the change in funding was the supplements, then we should have stayed steady around $6 million. But we didn’t.
Funding in 2018 dropped an additional 24%, the biggest single year decrease. The two year decrease from 2016 to 2018 was more than $3 million–a 40% decrease. This is an extraordinary number, hence my call for life support. Why did funding drop that second year, and why by so much?
I think this may partially reflect the opportunity cost of the Research Center RFA. I mentioned this in 2017. The application process for the Research Centers was time- and labor-intensive, and researchers from different institutions were collaborating. If all those researchers had been submitting individual applications, we could have seen an avalanche of proposals. Instead, those grant-writing resources were channeled into the Center applications, and a majority of them were destined to be unsuccessful. I can’t say for sure without knowing who submitted applications and asking them whether there was such an opportunity cost, but it’s a reasonable hypothesis.
Unfortunately, this does not explain where we are in 2020. There are a number of researchers who are not working in or with the Centers. Are they all submitting proposals? Have they left the field? Why has extramural funding stayed flat since 2018? What is being done to correct this problem?
Research Center Cliff
There’s another problem on the horizon for ME/CFS research, and that is the potential end of the Research Centers. The Research Centers received 61% of the total funding in FY 2020. On average, the Centers receive a combined $7.2 million per year, a total of $28.6 million thus far.
However, the Research Center grants last for five years, and that’s it. The timing of funding disbursements and when the clock runs out is a little confusing. The key date is August 2022, when the projects will officially end.
The Research Centers are not automatically renewable. There will have to be new applications, either for renewals or for new Centers. And because the funding came through a dedicated RFA, NIH will probably have to issue a new RFA for Center applications. Based on our experience the last time around, I think it is safe to say that a new RFA will take time to prepare.
However, there has been no indication from NIH that a new RFA is in the works. Dr. Vicky Whittemore commented in this week’s ME/CFS Advocacy Call that, “We’re also discussing what comes next after the five-year funding period for the current Collaborative Centers.” That’s about as neutral a statement as possible.
What would ME/CFS funding look like if the Centers are not renewed?
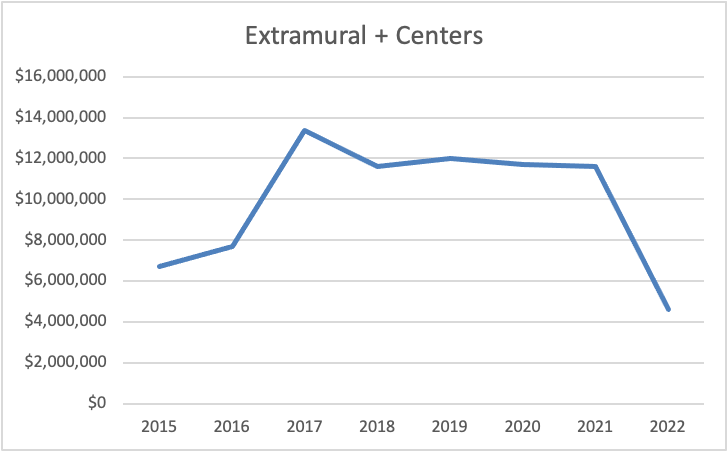
It looks terrible. It looks FRIGHTENING. Without the Centers, and without an increase in extramural funding, ME/CFS research funding would go from approximately $12 million to $4.5 million in one year.
Perhaps you’re thinking, “NIH won’t let that happen. They won’t kill the Centers.” I hope you are right. Just know that NIH did this once before. NIH funded several CFS research centers in the 1990s. By 2003, that funding was terminated, the Centers disbanded, and overall funding dropped 23% in a single year.
Today, the Centers represent such a huge proportion of the research portfolio that if NIH declined to renew them, our funding could drop by more than 60%. We are very very vulnerable as a result.
I think it would be foolish for NIH to abandon the Research Center strategy, especially given the likely explosion in the number of Americans diagnosed with ME in the next year or two. All of the time the Centers have spent building their infrastructure and cross-institution collaborations would be down the drain. But if we have learned nothing else about NIH, I hope we have learned that we cannot be complacent. It will take concerted effort and public pressure to secure just a renewal of the Centers, let alone an increase in their number or size.
A Confession
I’ll be honest, I am tired of writing posts about NIH funding where the bottom line is somewhere on a continuum between bad and worse. Even in 2017, our best year for funding ever, we only saw two new grants apart from the Research Centers. As soon as I scratch the surface and ask questions like “Is the field growing?” or “Is the slow seed strategy really working for us?” it becomes obvious that we are still in trouble.
The burden of disease in ME has always been among the highest of many chronic diseases, and NIH’s response has always been woefully behind. Now that we are starting to see Long COVID patients being diagnosed with ME, with more undoubtedly to follow, NIH’s failure to adequately fund ME research is foolish and unconscionable. If NIH had invested in ME/CFS research, we would have more answers. If we knew more, we could help people with Long COVID–or perhaps even prevent it. Instead . . . well, here we are.
Many people have worked incredibly hard to get ME funding to this point. I am proud to be among them. But I don’t feel a sense of accomplishment when I write these annual funding reviews. It has taken a staggering amount of effort–including physical effort by disabled people with ME–just to get us to this point. And where we are right now is not a good place. We still have a very long way to go.
Thanks for your analysis.
According to the organisers of the IACFS/ME meeting the small NIH funding can only be applied to in person meetings, so that will be used for the 2021 conference. Unless something changed after they posted this – see item 2.
https://www.s4me.info/threads/august-21-2020-iacfs-me-virtual-conference.15531/#post-274639
THANK YOU for the correction! I will update the post.
Thank you for your doggedness in getting this data and analyzing it for us!
I wish that the end results made the energy expenditure worthwhile (as in that the data showed improvement in funding).
And we are told repeatedly that we need to get funding ourselves and that if the right grants are submitted, they will be funded.
Thank you again for all that you do!
Just to clarify: Your 2019 report had intramural funding at just over $1M for both 2018 and 2019. Is it presumed to be at roughly the same level in 2020? If so, total ME funding for 2020 would then be close to $13M – essentially the same as 2019. Also, I assume intramural funding is included in the RCDC figures.
As explained in Note 1, intramural funding numbers will not be available for months. In the past, I have estimated the amount of intramural funding. However, this year I excluded it. All of the comparisons in the post, including the graphs, are for extramural grants and the Research Centers. That is true of 2020 and previous years as well. I removed the intramural funding so that I was comparing apples to apples.
Intramural funding is included in NIH’s RCDC (Research, Condition, and Disease Categorization) report of actual funding.
Pingback: Trial By Error: Jennie Spotila’s Annual Review of NIH Funding
Pingback: Trial By Error: Jennie Spotila’s Annual Review Of NIH Funding – The York ME Community